
With the Pfizer-BioNTech COVID-19 vaccine approval in the United Kingdom last week, and yesterday, in Canada, widespread vaccination programs are now ramping up in Europe and North America. It is worth noting (marveling, really) that we now have an authorized vaccine for a novel virus that was isolated less than a year ago. And so far, the data that have emerged on the efficacy of the major vaccine candidates has been impressive, far exceeding the modest expectations that many of us had when vaccination trials were launched several months ago.
Even before the pandemic there was a small but vocal anti-vaccine community, something that we at SBM have written about regularly since the blog’s inception. COVID-19 has paradoxically not silenced this group, but has accelerated and arguably grown their rhetoric to the point where widespread hesitancy to a COVID-19 vaccine has been reported in some countries. Amazingly, there are even those who still seem to believe that drugs like hydroxychloroquine are better than vaccination, because…vaccination is bad, apparently. And then there are those, like at least one US Senator, who seems to imply that a case of COVID-19 may actually be preferable to a vaccine. It’s like the measles parties, 2021 edition.
Concerns about vaccination may not be as uncommon as you might think, even when COVID-19 is killing thousands every day. With that in mind I developed a short table that might help the uncertain decide between the vaccine, getting a COVID-19 infection, and for the handful of people that still think it’s a useful COVID-19 therapy, hydroxychloroquine.
| The Vaccine (e.g., Pfizer-BioNTech) | A COVID-19 Infection | Hydroxychloroquine | |
| Active ingredient | nucleoside-modified messenger RNA (modRNA) encoding the viral spike glycoprotein (S) of SARS-CoV-2 | The SARS-CoV-2 virus | Hydroxychloroquine sulfate |
| Other ingredients | Lipids (to encase the RNA)
Salts (to balance the pH of the injection)
Other
|
None | Depends on brand, as generics are available.
One brand notes: Croscarmellose sodium, magnesium stearate, colloidal silicon dioxide, microcrystalline cellulose, hydroxypropyl cellulose, hydroxypropyl methylcellulose, polyethylene glycol, and titanium dioxide. |
| Preservatives | None | None | None |
| Been around since | 2020 | 2019 | 1955 |
| How many have received it | Over 40,000 in the clinical trial (over 20,000 received the vaccine) | As of December 9, 2020, approximately 68.7 million. | Based on the six trials I previously reviewed, 6,853 patients in RCTs, of which 2,619 received hydroxychloroquine. Before the COVID-19 claims appeared, it has a long history of use. Most COVID-19 use has been outside a clinical trial. |
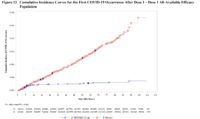
| Clinical effects | The chart from Pfizer’s briefing to the FDA is very impressive, where you can see (click to embiggen) efficacy appearing after only 14 days. Red line: cases in those that received placebo. Blue line: cases in vaccine recipients.
|
Varies from mild asymptomatic infection to severe disease with high mortality. Mortality rates vary by age, country, the presence of other diseases, etc. In the United States, the current case fatality rate is estimated at 1.9%. | Effective treatment for rheumatoid arthritis, systemic lupus erythematosus, and to prevent and treat malaria. Ineffective treatment for COVID-19. |
| Immunity efficacy (COVID-19) | Vaccine efficacy is estimated at 95% based on trial data reported to date.
|
N/A | None. All randomized controlled trials to date have shown no efficacy to prevent or treat COVID-19 infections. |
| Safety:
Short-term side effects |
Few differences between the vaccine and control group with exception of injection site reactions (pain, etc). Some severe immune reactions have been reported in the United Kingdom in two people with a history of severe reactions – this will need to be continued to be monitored. | Most people experience mild symptoms. Some will progress to severe disease and some of these patients become critically ill. Most people recover after 2-6 weeks. | Headache, nausea and vomiting, allergic reactions, hepatic problems, hair loss. |
| Long-term side effects | Still being evaluated. Most side effects of vaccines appear in the first 60 days (the data that we have to date) but very rare side effects may not be identified until the vaccine is administered to many millions of people. | The long term effects of COVID-19 infections may linger for weeks to months in some people. COVID-19 infections can damage the heart, lungs, and brain. Some complications are irreversible. Fatigue is most commonly reported, followed by cough, headache and body ache. Prolonged illness is possible, even in those without underlying medical conditions. In a group called “long haulers”, full recovery is uncertain. | Long list of effects including retinopathy and retinal toxicity, cardiomyopathy, skin reactions, neuromuscular effects, and other effects, some of which can be fatal. |
| Risk of Recurrence | Unclear. Most of the cases in the vaccine group occurred in the two weeks after administration of the first shot, which is the time when an immune response would be developing. The duration of the immune response remains unclear and will become apparent over time and with follow-up of the current clinical trials. However, it is possible that immunity from the vaccine will be long-lasting. | Unclear. Most of those infected with COVID-19 produce antibodies against the virus. Some seemingly rare cases of re-infection have been documented but the actual incidence remains unknown (but is probably very low). How long natural immunity will last is unclear. | Confers no protection against COVID-19. |
| Cost | Most health systems will be providing vaccines to citizens at no cost. | Free | A one-month supply should cost less than $30. |
{kind=link}
Conclusion: The SARS-CoV-2 vaccine could end the pandemic
Evidence that has emerged on the Pfizer-BioNTech and also the Moderna vaccine give us good reason to be cautiously optimistic, perhaps for the first time in this pandemic. The fact that both of these vaccines show such high rates of efficacy is reassuring: Immunization of populations against this disease appears possible. These are the earliest days with these vaccines, however and there is a long road ahead of safety monitoring and follow-up as these vaccines are offered to thousands, and then millions of people. We will also see additional trials report and additional vaccines move forward for regulatory approval. It is absolutely possible that there will be some adverse events identified that we haven’t seen yet. It is also very likely that vaccines will be blamed for events that are completely unrelated to the vaccine itself. But the alternative is killing thousands of people per day and injuring countless others, just in the United States alone, in a trend that continues to worsen with no end in sight. This is the largest logistical and immunization event of its kind in history. And we need it now.